115195
论文已发表
注册即可获取德孚的最新动态
IF 收录期刊
- 3.6 Breast Cancer (Dove Med Press)
- 4.3 Clin Epidemiol
- 2.6 Cancer Manag Res
- 3.2 Infect Drug Resist
- 4.1 Clin Interv Aging
- 6.1 Drug Des Dev Ther
- 4.1 Int J Chronic Obstr
- 8.7 Int J Nanomed
- 2.5 Int J Women's Health
- 3.2 Neuropsych Dis Treat
- 2.4 OncoTargets Ther
- 2.6 Patient Prefer Adher
- 2.6 Ther Clin Risk Manag
- 3.1 J Pain Res
- 3.5 Diabet Metab Synd Ob
- 4.5 Psychol Res Behav Ma
- 3.4 Nat Sci Sleep
- 2.4 Pharmgenomics Pers Med
- 2.6 Risk Manag Healthc Policy
- 4.6 J Inflamm Res
- 2.3 Int J Gen Med
- 3.9 J Hepatocell Carcinoma
- 3.3 J Asthma Allergy
- 2.5 Clin Cosmet Investig Dermatol
- 3.0 J Multidiscip Healthc

左心室射血分数与心力衰竭患者在冠状动脉造影或治疗后因造影剂诱发的肾病变和死亡率之间的关系
Authors Wang K, Li H, Bei W, Guo X, Chen S, Islam SMS, Chen J, Liu Y, Tan N
Received 21 March 2017
Accepted for publication 7 June 2017
Published 19 July 2017 Volume 2017:13 Pages 887—895
DOI https://doi.org/10.2147/TCRM.S137654
Checked for plagiarism Yes
Review by Single-blind
Peer reviewers approved by Dr Colin Mak
Peer reviewer comments 4
Editor who approved publication: Professor Deyun Wang
Background: Left
ventricular ejection fraction (LVEF) is the most widely used parameter to
evaluate the cardiac function in patients with heart failure (HF). However, the
association between LVEF and contrast-induced nephropathy (CIN) is still
controversial. Therefore, the aim of this study is to evaluate the association
of LVEF with CIN and long-term mortality following coronary angiography (CAG)
or intervention in patients with HF.
Methods: We
analyzed 1,647 patients with HF (New York Heart Association [NYHA] or Killip
class >1) undergoing CAG or intervention, including 207 (12.57%) patients
with reduced LVEF (HFrEF), 238 (14.45%) with mid-range LVEF (HFmrEF) and 1,202
(72.98%) with preserved LVEF (HFpEF). CIN was defined as an absolute increase
of ≥0.5 mg/dL or a relative increase of ≥25% from baseline serum creatinine
within 48–72 h after contrast medium exposure. Multivariable logistic
regression and Cox proportional hazards regression analyses were performed to
identify the association between LVEF, CIN and long-term mortality,
respectively.
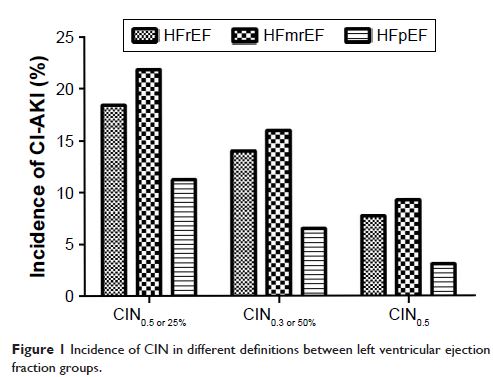
Results: Overall,
225 patients (13.7%) developed CIN. Individuals with lower LVEF were more
likely to develop CIN (HFrEF, HFmrEF and HFpEF: 18.4%, 21.8% and 11.2%,
respectively; P <0.001), but
without a significant trend after adjusting for the confounding factors (HFrEF
vs HFpEF: odds ratio [OR] =1.01; HFmrEF vs HFpEF: OR =1.31; all P >0.05). However, advanced HF
(NYHA class >2 or Killip class >1) was an independent predictor of CIN
(adjusted OR =1.54, 95% confidence interval [CI], 1.07–2.22; P =0.019). During the mean
follow-up of 2.3 years, reduced LVEF (HFrEF group) was significantly associated
with increased mortality (HFrEF vs HFpEF: adjusted hazard ratio =2.88, 95% CI,
1.77–4.69; P <0.001).
Conclusion: In
patients with HF undergoing CAG or intervention, not worsened LVEF but advanced
HF was associated with an increased risk of CIN. In addition, reduced LVEF was
an independent predictor of long-term mortality following cardiac
catheterization.
Keywords: cardiac
catheterization, contrast-induced nephropathy, left ventricular ejection
fraction, heart failure